
Cannibalization isn’t the Only Possibility
Cannibalization isn’t the Only Possibility
This piece was originally written as a response to a discussion on Marginal Revolution regarding the economic influence nursing agencies and nursing agency-like companies have on healthcare professionals.
We’ve recently seen some writing remarking on the relatively large changes the nursing labor market has been going through in the last couple years. Spurred by Covid, there have been some massive changes in the way nurses find work and maintain employment that have been started to be noticed in places like Marginal Revolution, which prints Andrew K. Stein’s thoughts on the nursing market:
What’s happening in the labor market, I think, is that there are two paths for a bedside nurse in the COVID era — keep working for a hospital or go work for an agency. Agency pay has gotten ridiculously high, so more and more nurses are quitting the local hospital, signing on with the agency, and then going to work for any hospital that can pay the agency’s rates. In exchange for going wherever the highest bidder is, they get huge increases in their take-home pay. No shame in that.
The net effect, I suspect, is that the bargaining power of nursing labor is going way up, though with unequal gains; to benefit, you have to quit your hospital-employed job and be willing to go wherever the agency sends you.
And then your open slot gets backfilled by another agency nurse from somewhere else!
It’s a reinforcing cycle: As nursing shortages rise, nurses increasingly “work short” — i.e., caring for more patients per shift than is reasonable — or work more shifts per week than typical. That daily stress spurs many nurses to either leave the bedside for something more 9-to-5 (think outpatient clinics) or jump into travel nursing to at least get paid for the extra load everyone is being forced to bear right now.
Agencies and travel nurses win, hospitals and hospital-employed nurses lose.
Andrew’s thoughts are correct in a lot of ways here, but incorrect on others and only technically correct for a few. Despite technical correctness reputedly being the best kind of correct, we think it’s worthwhile to put our two cents in because the real picture is a bit more complex.
The misvalued market
One place where Andrew is correct is that the bargaining power of nursing has way up. Our country’s nursing shortage is by no means new, and a large shortage of labor usually (and rightfully) results in a large increase in pay. But the confusing bit here is that the increased demand doesn’t seem to drive the increased bargaining power as we’d expect. For instance, here’s a chart showing year-over-year stagnation in wages for all nursing titles from 2019 to 2029:
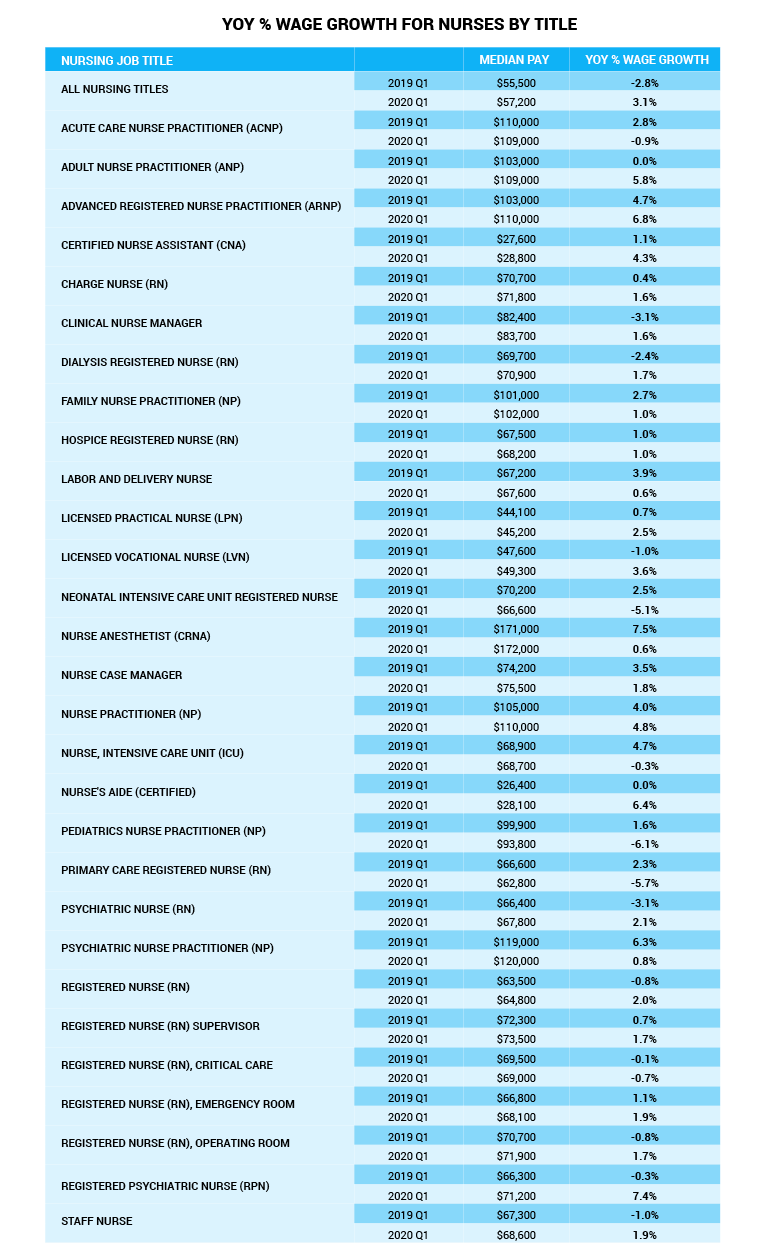
There’s some complexity in that article that attempts to explain why wages aren’t going up as you’d expect them to (for instance, money-making procedures being performed less), but one thing seems clear - they aren’t skyrocketing, and demand has.
When you combine the fact that demand is ever-growing and that wages aren’t growing to meet it and that this in and of itself didn’t increase “negotiating power”, we are now in a situation where something like an oligarchy is implied - somehow these nurses are worth more than the wage they are getting, but nobody is agreeing to give it to them. It isn’t necessarily true that there’s collusion going on here, but something is; there’s some kind of roadblock keeping the market from acting as we’d expect.
This is only strengthened by the fact that when you allow the nurses to actually ask for the wages they seem to be worth outside of the standard hiring process, the health care facilities actually do it. The nurse’s value was higher the whole time; he or she just wasn’t seeing all of that value, because they didn’t have a compelling, powerful way to enable people to bid for them. That’s where we come in: we allow for that.
Another implication of the piece I’d like to address is that other nurses who still work in hospitals are necessarily the losers here; this isn’t impossible, but it’s far from clear and also not what we’d expect as a long term result of nurses, in general, gaining the ability to market themselves more effectively. In the scenario described, Andrew K. Stein draws a picture of healthcare facilities using agency nurses not only because they are convenient, but also because they sometimes have to; there’s a labor shortage, and they have to have the labor. But if that’s the case, you wouldn’t expect the pay nurses that work at health care facilities to remain the same indefinitely.
To the extent health care facilities value having nurses in a traditional employee-employer relationship, they will eventually have to adjust how they pay them to be competitive, whether they like it or not. If the healthcare facilities don’t value employment-over-agency models for any reason other than the ability to pay them less, this means eventually they’d abandon the model entirely for the sake of the increased flexibility of the agency model. But to the extent they value anything else - familiarity with particular nurses, consistency, etc. - they will eventually have to raise the amount they are willing to pay for it to be competitive.
Note that the same kinds of pressures affect the agency-vs-employment decision on the nurses’ side of things; they are balancing consistency of work and the amount of their own effort has to be spent to find/coordinate it as well as other more traditional aspects of this kind of decision like health benefits. On both sides, there’s an idea of balance - each side trying to get the most they can while still having people who will take the deal they offer. That’s not unusual at all. In fact, it’s a pretty good summary of how a healthy, fair market works.
Stein seems to think that agency nurses as a whole are putting health care facility-employed nurses at a disadvantage by taking advantage of the flexibility and pay advantages agencies provide. He puts it this way:
It’s a reinforcing cycle: As nursing shortages rise, nurses increasingly “work short” — i.e., caring for more patients per shift than is reasonable — or work more shifts per week than typical. That daily stress spurs many nurses to either leave the bedside for something more 9-to-5 (think outpatient clinics) or jump into travel nursing to at least get paid for the extra load everyone is being forced to bear right now.
Agencies and travel nurses win, hospitals and hospital-employed nurses lose.
His argument makes superficial sense, but it gets a little more complex the closer you look. For instance, he lists two destinations nurses leave conventional hospital employment for - outpatient clinics and agencies. But of the two, only one necessarily implies lower total hours, and it’s not the agency. Agency nurses might work fewer hours, but they don’t necessarily; many of our nurses are working extra time on top of their normal schedules for a variety of reasons ranging from extra income to just seeing what’s out there in terms of jobs and workplaces. In their case, they are additive to the labor supply rather than diminishing it.
Even where they do work fewer hours, this is still indicating a market mismatch that isn’t created by them or the agencies - where someone isn’t willing to take on a marginal work hour, we normally understand it’s because they value that hour more than the pay being offered. Where they don’t value that hour more than the pay, we understand something else is up - usually that the nurse would rather not work that hour for the pay offered, but has to for some other reason (say, fear of losing their job if they don’t). Again, we find a situation that makes a lot more sense if you think of it as a return to economic homeostasis - where pay was lower than it should be, it has now (for some) corrected. Where hours were longer than the pay justified, they are now (for some) shorter, or else compensated at their actual worth to the worker.
I previously mentioned that agency nurses don’t just improve their own leverage in the market by accessing agencies and apps like CBH’s, but instead improve the negotiating power of all nurses. While this is true, we’d also expect an even bigger benefit in the long term: by increasing their own pay, they are increasing the average pay of nurses overall. In a traditional market model, we would expect this to draw more and more towards nursing. There are a lot of factors here that might slow this down (nursing school capacity might lag, for instance) but we’d still expect this to help nursing supply long term, not hurt it.
Overall Stein’s argument has to do with winners and losers, positing that nurses at health care facilities (and the facilities themselves) lose out where others win. But in the long term, we think everyone wins here - nurses who choose to go the agency route gain access to the ability to get market rates for their work, health care facilities get increased staffing flexibility (and eventually an even greater supply of nurses) and nurses who remain employed at healthcare facilities have more of the leverage they need to increase their pay and improve their working conditions. Far from being injurious to the market and harmful to half of its participants, We think the long-term effects of nursing agencies will be that - just as you’d expect any time barriers to the proper function of markets are removed - that nearly everyone wins, and potentially wins big.